Key Takeaways
-
TENS primarily modulates pain through nerve stimulation rather than directly relaxing muscles; muscle relaxation is an indirect secondary effect that occurs when pain and protective muscle guarding decrease.
-
Frequency settings critically determine TENS effects: low frequencies (<10 Hz) at higher intensity can induce muscle contractions and endorphin release, while high frequencies (>50 Hz) at low intensity produce sensory tingling without contractions.
-
EMS/NMES is fundamentally different from TENS and is the appropriate modality when active muscle contraction, strengthening, or muscle re-education is the clinical goal.
-
Electrode placement directly affects therapeutic effectiveness; proper positioning relative to nerve pathways and the pain site, with consideration for dermatome mapping, is essential for optimal outcomes.
-
Clinical TENS sessions typically range 15-60 minutes with frequency varying by condition; overuse causes neural adaptation and reduced efficacy, requiring standardized protocols based on condition type.
-
TENS carries minimal risk when protocols are followed, with contraindications including pacemakers, pregnancy over abdomen/lower back, open wounds, and areas lacking sensation.
One of the most common questions clinicians encounter from patients and colleagues alike is: does a TENS unit relax muscles? The answer is nuanced, clinically important, and directly affects how healthcare providers select and deploy electrotherapy modalities. Whether you operate a physical therapy clinic, a chiropractic practice, or an auto accident injury center, understanding the precise mechanism of transcutaneous electrical nerve stimulation (TENS) can improve patient outcomes and sharpen your treatment protocols.
TENS is a noninvasive electrotherapy modality that delivers low-voltage electrical impulses through electrodes placed on the skin to interact with nearby nerve pathways. According to the Cleveland Clinic, pain relief often begins immediately during a session but typically dissipates within about one hour after the device is turned off. This time-limited effect has significant implications for how providers integrate TENS into broader treatment plans. The following 13 points outline what every clinician should understand about TENS and muscle relaxation.

1. TENS Primarily Targets Nerve Pathways, Not Muscle Tissue
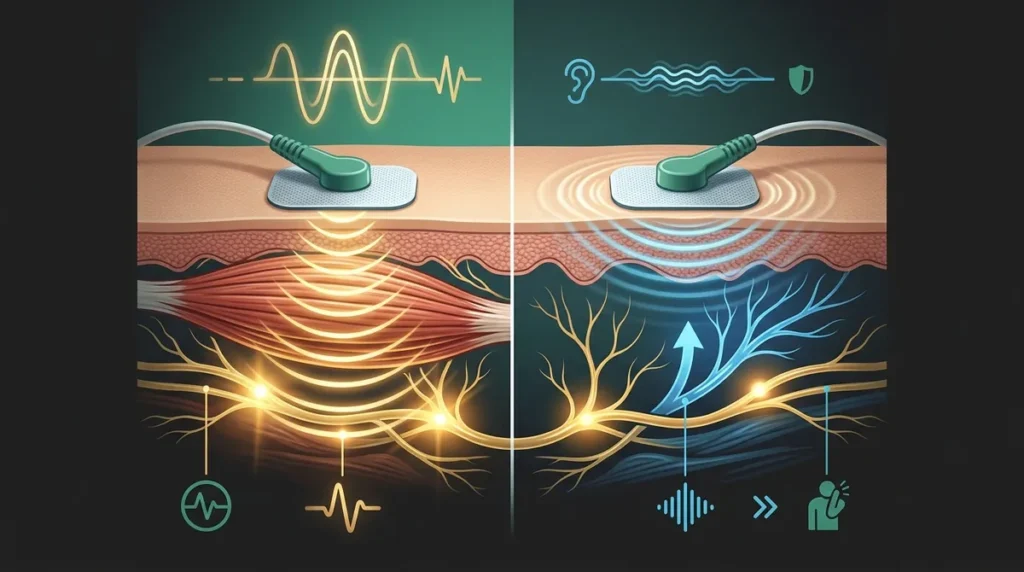
The foundational principle of TENS therapy is pain modulation via nerve stimulation, not direct action on muscle fibers. The device delivers electrical impulses that interact with sensory nerve pathways, altering the way pain signals are transmitted to the brain. This distinction is critical when advising patients who expect TENS to function like a muscle relaxant medication.
2. Muscle Relaxation Is Often an Indirect Effect
When pain is reduced through TENS, the muscles that were guarding or tensing in response to that pain often begin to release. This indirect relaxation effect can be clinically meaningful, particularly in patients with chronic back pain or post-injury muscle tightness. However, clinicians should be precise: the relaxation is a secondary response to pain relief, not a primary physiological mechanism of TENS itself.
3. Frequency Settings Determine Whether Muscle Contraction Occurs
According to StatPearls via the National Institutes of Health, TENS delivered at low frequencies (below 10 Hz) at higher intensities can induce muscle contractions, while high frequencies (above 50 Hz) at low intensity produce tingling sensations without contractions. This frequency-dependent behavior is essential knowledge for providers calibrating devices for specific therapeutic goals. Selecting the wrong frequency range can produce unintended outcomes.
| Frequency Range | Intensity Level | Primary Effect | Clinical Application |
|---|---|---|---|
| Low (<10 Hz) | Higher | Muscle contractions possible | Endorphin release, deep pain relief |
| High (>50 Hz) | Lower | Sensory tingling, no contractions | Gate control pain modulation |
| Burst Mode | Variable | Intermittent stimulation | Combines effects of both ranges |
4. TENS and EMS Are Fundamentally Different Modalities
A common source of confusion in clinical settings is the interchangeable use of TENS and electrical muscle stimulation (EMS), also known as neuromuscular electrical stimulation (NMES). EMS/NMES is specifically engineered to produce muscle contractions for strengthening, muscle re-education, and spasm management. TENS, by contrast, is designed primarily for pain relief. Providers looking to actively contract or retrain muscles need a different electrotherapy modality entirely. To explore the full range of available products for your clinic, reviewing a comprehensive electrotherapy catalog is strongly advised.
| Modality | Primary Goal | Mechanism | Causes Muscle Contraction? |
|---|---|---|---|
| TENS | Pain relief | Nerve stimulation / gate control | Rarely (only at low frequency/high intensity) |
| EMS/NMES | Muscle contraction & rehab | Motor nerve stimulation | Yes, by design |
| Interferential (IFC) | Deep tissue pain & edema | Intersecting medium-frequency currents | Possible at certain settings |
5. Conditions That Benefit Most From TENS Therapy
TENS is commonly indicated for conditions involving nerve-mediated pain, including osteoarthritis, tendinitis, fibromyalgia, and chronic back pain. Auto accident injury clinics frequently use TENS to address whiplash and soft tissue injuries, where pain and secondary muscle guarding are prevalent. Understanding the appropriate diagnostic context helps providers match patients to the correct electrotherapy intervention. For further clinical guidance, the article on what TENS units actually do for clinical pain management offers a detailed breakdown.
6. The Gate Control Theory Explains the Pain-Relaxation Connection
The gate control theory of pain, foundational to understanding TENS, proposes that non-painful sensory input (such as electrical stimulation) can close the neural “gate” to painful signals traveling to the brain. When pain signals are blocked or diminished, the reflexive muscle tightening associated with pain responses naturally decreases. This neurophysiological pathway is why many patients report feeling both less pain and less muscle tension after a TENS session, even though the device is not directly relaxing the muscles.
7. Electrode Placement Is Critical to Achieving Desired Outcomes
The therapeutic effectiveness of a TENS session depends heavily on where electrodes are placed relative to the nerve pathways and the area of discomfort. For back pain, electrodes are typically positioned on either side of the spine near the affected spinal segment. For extremity pain, placement near the peripheral nerve supplying the affected region is preferred. Clinical resources such as the electrotherapy electrodes clinical guide for providers offer evidence-based placement protocols that can standardize care across your clinical team.
Proper electrode placement considerations include:
- Positioning electrodes proximal to the pain site for nerve pathway access
- Avoiding placement over joints, broken skin, or sensitive tissue
- Using adequate electrode-to-skin contact to prevent burns or irritation
- Considering dermatome mapping for radicular or referred pain patterns
8. Evidence for TENS Effectiveness Is Mixed but Growing
Clinicians should approach TENS with informed expectations. A 2019 Cochrane review found insufficient evidence to either support or reject TENS for chronic pain, and the CDC recognizes nonopioid therapies like electrotherapy as important components of multimodal pain management. Some studies indicate a placebo effect may account for a portion of perceived benefits. Despite this, TENS remains widely used in clinical settings because it carries minimal risk, is noninvasive, and aligns with current guidance favoring non-pharmacological pain interventions.
9. TENS Is Generally Low-Risk When Protocols Are Followed
According to StatPearls, complications from TENS are minimal when the device is used within manufacturer parameters. The most commonly reported adverse effects include mild skin irritation beneath electrodes, uncomfortable tingling at high intensities, and rare electrode-related burns. Clinicians should always instruct patients on proper device use and review contraindications, which include pacemaker use, pregnancy (over the abdomen or lower back), and application over open wounds or tumors. Reviewing what the TENS unit pads actually do for pain relief can help providers counsel patients on safe application.
Key safety contraindications for TENS include:
- Implanted cardiac devices (pacemakers, defibrillators)
- Active malignancy over the stimulation site
- Pregnancy (particularly the abdomen and lower back)
- Open wounds, rashes, or compromised skin integrity
- Lack of sensation in the electrode area (neuropathy risk)
10. Conductive Garments Can Enhance TENS Delivery for Muscle Areas
One advancement in clinical TENS application is the use of conductive garments, which distribute electrical stimulation more evenly across larger muscle groups and body regions. Unlike traditional adhesive electrode pads, conductive garments conform to the body’s contours and are particularly effective for treating larger areas such as the lower back, shoulders, and thighs. This broader stimulation coverage can enhance the indirect muscle relaxation effect by addressing pain more comprehensively across the affected region.
11. Back Braces Complement TENS for Spinal Muscle Pain
For patients with chronic lumbar pain and associated paraspinal muscle tension, combining TENS therapy with appropriate spinal support can improve outcomes. Back braces reduce mechanical load on the spine and surrounding musculature, decreasing the pain stimulus that TENS is working to modulate. This integrative approach is particularly valuable in chiropractic and physical therapy settings where multimodal treatment protocols are standard. Providers can refer to the guide on how to choose the best TENS unit for your clinical practice when building comprehensive patient care packages.
12. Session Duration and Frequency Affect Therapeutic Outcomes
Clinical TENS sessions typically range from 15 to 60 minutes, depending on the condition being treated and the patient’s tolerance. The FDA has encouraged the use of nonopioid pain management strategies, and optimizing TENS session parameters is an important component of achieving durable results. Overuse or excessively long sessions can reduce efficacy through neural adaptation, where the nervous system becomes desensitized to the stimulus. Establishing standardized protocols based on condition type and patient response supports consistent outcomes.
Recommended session parameters by condition type:
| Condition | Suggested Session Duration | Frequency per Week | Preferred TENS Mode |
|---|---|---|---|
| Chronic low back pain | 20–45 minutes | 3–5 times | High frequency conventional |
| Post-injury soft tissue pain | 15–30 minutes | 2–4 times | Burst or conventional |
| Fibromyalgia | 30–60 minutes | Daily as tolerated | Low frequency acupuncture-like |
| Whiplash/auto injury | 20–30 minutes | 3–5 times | Conventional high frequency |
13. Selecting the Right Electrotherapy Device Matters for Clinical Results
Not all TENS devices are created equal. Clinical-grade TENS devices offer programmable frequency ranges, multiple channel outputs, and adjustable waveform parameters that enable clinicians to precisely tailor therapy. Consumer-grade devices often lack the granularity required for professional applications. Resources such as what makes the best TENS machine for clinical use can guide procurement decisions. Physical therapy clinics, chiropractic offices, and auto accident injury centers should prioritize devices that support multi-patient use, offer durable construction, and come backed by insurance-compatible documentation processes.
Liberty Medical Solutions specializes in customized electrotherapy solutions for clinical providers, offering a range of TENS devices, back braces, conductive garments, and cervical traction units. The company also works with commercial PPO/POS plans, workers’ compensation, and auto accident claims to ensure providers and patients can access the equipment they need without unnecessary financial barriers. For additional decision-making support, the physical therapy equipment electrotherapy guide for clinics is an excellent reference for building or expanding a clinic’s modality inventory.
To summarize key clinical takeaways:
- TENS primarily modulates pain through nerve stimulation, not direct muscle relaxation
- Indirect muscle relaxation occurs as a secondary response when pain is reduced
- EMS/NMES is the appropriate modality when active muscle contraction is the goal
- Device selection, electrode placement, and frequency calibration are critical to efficacy
- TENS is a low-risk, noninvasive tool that aligns with current non-opioid pain management guidance
Conclusion
Understanding whether a TENS unit relaxes muscles requires a precise grasp of electrotherapy mechanisms and their clinical distinctions. TENS is a powerful pain modulation tool that can indirectly reduce muscle tension by addressing its root cause — pain and the protective guarding responses it triggers. For providers seeking to optimize patient outcomes, selecting the right electrotherapy device, applying correct protocols, and integrating TENS within a broader multimodal strategy are all essential steps. The nerve stimulators in electrotherapy clinical guide for providers is a valuable resource for deepening your clinical knowledge base.
If you are ready to expand your clinic’s electrotherapy capabilities or need guidance on sourcing the right TENS devices, back braces, or conductive garments for your patient population, reach out to our clinical solutions team at Liberty Medical Solutions to discuss customized options tailored to your practice’s specific needs.
FAQs
Q: Does a TENS unit directly relax muscles?
A: A TENS unit does not directly relax muscles. Its primary function is pain modulation through nerve stimulation, and any muscle relaxation that occurs is typically an indirect result of reduced pain and the corresponding decrease in protective muscle guarding.
Q: What is the difference between TENS and EMS for muscle treatment?
A: TENS (transcutaneous electrical nerve stimulation) is designed for pain relief through nerve pathway modulation, while EMS or NMES (neuromuscular electrical stimulation) is specifically engineered to produce motor nerve activation and muscle contractions. Clinicians should select the appropriate modality based on whether the treatment goal is pain management or active muscle contraction and rehabilitation.
Q: Can TENS therapy help with muscle spasms?
A: TENS may provide indirect relief for muscle spasms by reducing the pain that often accompanies or triggers them. However, EMS or NMES is generally considered the more targeted modality for directly addressing muscle spasm through controlled electrical stimulation. Providers should evaluate the underlying cause before selecting the appropriate electrotherapy intervention.
Q: How long does a clinical TENS session typically last?
A: Clinical TENS sessions generally range from 15 to 60 minutes, depending on the condition being treated, the patient’s tolerance, and the clinical protocol in use. Session duration and frequency should be calibrated to avoid neural adaptation, which can reduce the effectiveness of the therapy over time.
Q: Is it safe for patients to use a TENS unit every day?
A: Daily TENS use is generally considered safe for most patients when the device is operated within manufacturer-specified parameters and appropriate contraindications are observed. However, clinicians should monitor for signs of skin irritation beneath electrodes and assess whether session frequency needs adjustment based on patient response and therapeutic progress.

